Infection Control in MRI and CT Diagnostic Centers
What patients, clinicians, and facility managers need to know about the microbial world lurking inside your scanner room
Millions of patients pass through MRI and CT scanner rooms every year, lying on the same tables, breathing the same air, and pressing their bodies against the same surfaces as dozens of strangers before them. Cancer patients on chemotherapy, people living with HIV/AIDS, organ transplant recipients on immunosuppressants — the very patients who most urgently need diagnostic imaging are also those whose immune systems are least able to withstand an encounter with a stray pathogen.
Yet, despite decades of intensive research into infection control in surgical theatres and intensive care units, the humble radiology department has remained something of a hygiene blind spot. No international standards govern MRI scanner cleanliness. Routine disinfection between patients is, in many centres, essentially unheard of. And the sources of contamination are far more varied — and sometimes far more surprising — than most people assume.
This article brings together findings from peer-reviewed research to map the true scope of the infection risk inside diagnostic imaging facilities, from the expected to the frankly counterintuitive — including why a dog in the scanner room might actually be a sign of superior hygiene, and why the doctor’s necktie dangling over your face during an examination may be more dangerous than you think.
1. The Radiology Department as a Microbial Crossroads
Radiology departments occupy a peculiar position in the hospital ecosystem. Unlike the operating theatre — sealed, scrubbed, and governed by strict aseptic protocols — or the ward, where infection control nurses make daily rounds, the radiology suite tends to operate like a busy railway station: high throughput, constantly shifting populations of patients, and no single owner responsible for ensuring cleanliness between each passing train.
The sheer diversity of patients passing through compounds the problem. A morning slot in a busy MRI suite might include an elderly patient with an infected diabetic ulcer, a young athlete with a sports injury, a neutropenic cancer patient recovering from their third round of chemotherapy, and a child with suspected appendicitis. Each person deposits their own microbial signature on the surfaces they touch. Each person may pick up whatever the previous occupant left behind.
“A variety of patients pass through the radiology department, patients prone to infections, asymptomatic carriers, and patients with clinical infections. This places high demands on the cleaning of the machines between patients.” — Surface Contamination of CT and MRI Equipment, ScienceDirect (2019)
Research from Stockholm, published in a landmark 2019 study in the radiology literature, sampled ten predetermined surfaces inside and outside CT and MRI examination rooms across six public and four private radiology departments. Bacterial colony-forming units were found on virtually all surfaces examined. The highest bacterial burdens were recovered from keyboards, chairs in patient changing rooms, headphones, and the alarm buzzer patients squeeze to communicate with the technologist. These are exactly the surfaces that receive the most direct hand contact — and are least likely to be wiped down between patients.
What lives on your scanner?
The organisms most commonly found in radiology environments span a troubling range. Gram-negative bacteria including Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii have been isolated from X-ray equipment surfaces. These organisms can adhere tenaciously to the plastic and metal components of imaging equipment and survive there for two weeks or longer, calmly waiting for their next host.
MRSA — methicillin-resistant Staphylococcus aureus, the bacterium that has come to epitomise the crisis of antibiotic resistance — has been found to colonise MRI machines with particular enthusiasm, and can survive on surfaces such as mattress pads for up to eleven or twelve days. It is estimated that up to 53 million people worldwide carry MRSA asymptomatically, meaning patients with no signs of infection can seed a scanner room with drug-resistant bacteria entirely without knowing it.
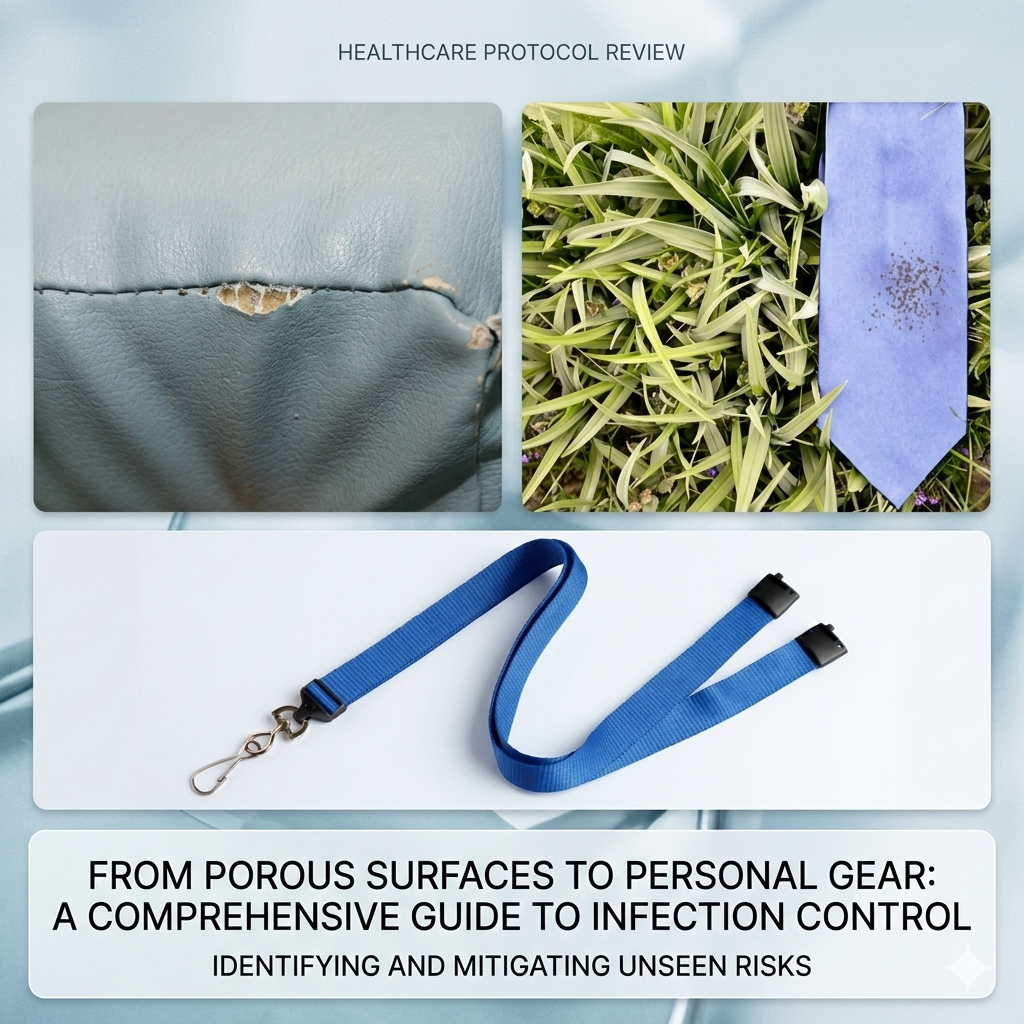
The scanner bore itself — the tunnel through which the patient passes — presents a particular challenge. Because of the powerful magnetic field and the delicate electronics, cleaning crews are often restricted from entering the MRI suite. As a result, many MRI scanner bores are rarely, if ever, properly cleaned. The padding on imaging tables, designed in an era before MRSA was a significant concern, is frequently worn, frayed, and harbours moisture in its foam core — conditions bacteria find extremely hospitable.
An Italian study reported that 41.7% of X-ray tubes and 91.7% of control panels and imaging plates in radiology rooms were contaminated — and bacteria found on X-ray machines can survive on plastic and metal surfaces for more than two weeks. (ISID Guide to Infection Prevention and Control in the Radiology Department, 2021)
The CT wrap — the padded foam sleeve used to immobilise patients during CT scans — has been identified as the single most contaminated item on a CT scanner in a study by researchers at a major quaternary care hospital. Iterative cleaning and disinfection quality improvement cycles were required before contamination was brought under acceptable control.
2. The Surprising Suspects: Beards, Ties, and Lanyards
The beard study that made headlines
In 2018, a research group in Switzerland published what became one of the most-shared papers in the history of radiology — not because it confirmed what everyone suspected, but because it overturned it entirely.
The study, led by Dr. Andreas Gutzeit and colleagues and published in European Radiology, set out to determine whether it was safe for dogs and humans to share the same MRI scanner. Concerns about zoonotic infections — diseases transmissible from animals to people — had made many radiology departments refuse to allow dogs to use their equipment, even in regions with a desperate shortage of veterinary MRI facilities.
Gutzeit’s team compared bacterial colony-forming units from 18 bearded men and 30 dogs attending a radiology department in Lucerne, Switzerland. The results were stunning. Every single man tested — 100% of them — had a high microbial count on their beards. Only 77% of dogs carried a comparably high bacterial load. More strikingly, human-pathogenic bacteria were found in the beards of 7 out of 18 men (39%), versus just 4 out of 30 dogs (13%) in their fur. The organisms found in human beards included Enterococcus faecalis and Staphylococcus aureus — both dangerous opportunistic pathogens in vulnerable patients.
The conclusion was blunt: bearded men harbour significantly higher bacterial burdens, and more human-pathogenic strains, than dogs. On pure hygiene grounds, having a dog in the scanner may be less risky than having a bearded radiologist lean over the equipment.
The study also contained a quietly devastating observation about routine disinfection practices. When the MRI scanner shared with dogs was sampled after thorough disinfection with an alcohol-free disinfectant wipe — a process that took just two minutes — mean bacterial colony counts on the table and coils dropped to essentially zero. The same scanner, during routine human clinical use without scheduled disinfection, carried mean counts of five to seven CFUs per plate. Human-only scanners at two comparison institutions showed similar contamination during normal clinical use, and in two cases harboured Staphylococcus aureus on their receiver coils.
The punchline is profound: because dog examinations triggered a mandatory disinfection protocol, the scanner used by dogs was actually cleaner than scanners used exclusively by humans. This finding alone should prompt every radiology department manager in the world to ask when their equipment was last properly disinfected.
The necktie: a mobile petri dish
The humble physician’s necktie has long been suspected as a potential vehicle for infection. It hangs freely at the front of the body, brushing against patients during examinations, rarely laundered, and excluded from the hand-hygiene protocols that govern direct patient contact.
The evidence is not without nuance. A systematic review published in CMAJ Open in 2018, which examined all relevant studies published between 1966 and 2017, found limited but real evidence that neckties are contaminated with pathogenic bacteria — including MRSA — and very limited but mechanistically plausible evidence that they can transmit bacteria to patients. A study at the New York Hospital Medical Center found that nearly half of the neckties worn by surgical clinicians harboured potentially infectious pathogens. A London study found significantly higher bacterial counts on doctors’ ties compared to their shirt pockets, with the difference attributable to one obvious factor: ties are washed far less frequently than shirts.
An experimental study published in the Journal of Hospital Infection attempted to quantify the risk more precisely. A physician wearing a tie artificially inoculated with the test organism Micrococcus luteus simulated routine patient examinations on mannequins. Of ten mannequins examined while the physician wore a contaminated tie, six tested culture-positive. Only one of ten mannequins was contaminated without the tie. The tie, in this controlled experiment, increased bacterial transfer to patients six-fold.
As Andrew Frei wrote in the Journal of Community Hospital Internal Medicine Perspectives: neckties “frequently come into contact with germs and human secretions, becoming mobile petri dishes that follow the wearer everywhere.”
The United Kingdom’s Department of Health concluded, as part of its ‘bare below the elbows’ dress policy, that it is poor practice for clinicians to wear neckties during direct patient care. The policy acknowledges the evidence is not definitive, but operates on the principle that when a risk factor can be easily eliminated at no cost, and the potential benefit is real, eliminating it is the rational choice.
The same logic applies to lanyards — the fabric loops worn around the neck to carry hospital ID badges. Research has isolated methicillin-sensitive Staphylococcus aureus, MRSA, and Enterococcus species from lanyards and badges worn by healthcare workers. A higher bacterial load was noted on lanyards compared to badges, presumably because the fabric traps moisture and organic material more effectively than a plastic card. In the context of a radiology department, where the lanyard may brush against scanner equipment, patient tables, or contrast injection ports throughout the day, this represents a plausible if underappreciated vector of cross-contamination.
3. Viral Infections: The Less-Studied Dimension
While bacterial contamination has attracted most of the research attention in radiology infection control, viral pathogens present a distinct and serious threat — particularly for immunocompromised patients who may be unable to mount effective responses to viral challenges that healthy individuals would handle without difficulty.
Hepatitis C transmission within radiology departments has been documented in multiple case studies. In several reported outbreaks, breaches in safe injection practices — including the contamination of shared intravenous contrast media vials — were identified as the source. In one modelling study published in PLoS One, researchers calculated that microliter volumes of contaminated blood were sufficient to seed an outbreak of hepatitis C during CT examinations, highlighting how vanishingly small the infectious dose can be.
The automated contrast injectors used in CT and MRI examinations have themselves been identified as a potential contamination source. A 2019 German study found bacterial contamination in automated MRI contrast injectors during routine clinical use — equipment that delivers a substance directly into the patient’s bloodstream.
Mobile phones carried by radiographers and radiologists represent another underappreciated vector. Research has demonstrated that healthcare workers’ phones carry bacterial and viral contamination, and that they are rarely if ever disinfected. A British study specifically examining radiographers found that mobile phone use in clinical areas was common, and that an awareness campaign was only modestly successful at changing behaviour.
4. The Immunocompromised Patient: Heightened Stakes
For the general population, exposure to MRSA on a scanner table or Enterococcus from a physician’s necktie might result in nothing more serious than a skin infection — unpleasant, but treatable. For a patient whose immune system has been deliberately or inadvertently suppressed, the same exposure can be catastrophic.
Cancer patients undergoing chemotherapy
Chemotherapy drugs kill cancer cells by targeting the fastest-dividing cells in the body — but they cannot distinguish between cancer cells and the bone marrow cells that produce infection-fighting white blood cells. The result is chemotherapy-induced neutropenia: a state in which the absolute neutrophil count falls to dangerously low levels, stripping the patient of their primary line of defence against bacterial invasion.
The incidence of sepsis among cancer patients is approximately 16.4 cases per 1,000 patients per year, with in-hospital mortality approaching 38% in severe cases. Infections are among the leading causes of death in cancer patients, with a fatal infection rate approximately three times higher than in the general population. The organisms responsible are not exotic: Escherichia coli, Pseudomonas aeruginosa, Klebsiella species, Staphylococcus species, and Streptococcus species — exactly the bacteria routinely found on radiology equipment.
The CDC makes the point with clarity: “Infection during chemotherapy can lead to hospitalization or death.” Yet cancer patients undergoing chemotherapy frequently require CT scans to monitor treatment response, MRI examinations to assess their tumours, and nuclear medicine studies to evaluate metabolic activity. Each visit to the radiology department is both medically necessary and a potential encounter with infection.
Almost all microorganisms can cause infection in cancer patients, including those which form part of normal human microbiota. This is the landscape of risk that neutropenic patients bring with them to the scanner room — a world where the otherwise harmless becomes lethal.
HIV/AIDS patients
People living with HIV, particularly those not yet established on effective antiretroviral therapy or with persistent low CD4 counts, face susceptibility to a broader range of opportunistic pathogens than the general population. Fungal organisms such as Cryptococcus and Pneumocystis jirovecii, bacteria like Mycobacterium avium complex, and viral pathogens including cytomegalovirus can all cause life-threatening infections in HIV-positive individuals that would cause minimal harm in an immunocompetent person.
The risk landscape changes further when HIV infection coexists with malignancy or transplantation, both of which require their own immunosuppressive burdens. CT and MRI remain the primary imaging modalities used to diagnose and monitor opportunistic infections in these patients — which means the very equipment used to detect their infections must be maintained to the highest hygiene standards to avoid causing new ones.
Organ transplant recipients
Transplant recipients require long-term immunosuppression to prevent rejection of their new organ. This places them in a state of indefinite vulnerability to infection — not just in the immediate post-transplant period, but for the rest of their lives. A single inadvertent exposure to a drug-resistant organism acquired from a contaminated scanner table could initiate a cascade leading to septic shock, organ failure, and death.
The irony is stark: transplant patients are among the heaviest users of MRI and CT services for their ongoing medical monitoring, and they are simultaneously among those least able to withstand the infectious consequences of inadequate radiology hygiene.
5. The Systemic Problem: No Standards, Inconsistent Practice
One of the most troubling findings from the research literature is not any specific source of contamination, but the fundamental absence of a framework to address them.
There are currently no international standards governing MRI hygiene in clinical practice. How often should scanner tables be wiped? What agent should be used? What surfaces require attention between each patient, versus at the end of the day, versus at the end of the week? These questions do not have agreed answers. Individual hospitals and radiology departments formulate their own policies, which vary enormously in their stringency and in whether they are actually followed.
The estimated annual cost of healthcare-associated infections in US hospitals alone ranges from $28 billion to $45 billion. An estimated 1.7 million patients per year in the United States acquire a healthcare-associated infection — and approximately 100,000 of those patients die. Nearly all HAIs are preventable.
A survey finding that 88% of radiographers felt that lack of regular disinfection was a major contributing factor for contamination of radiology equipment is telling. The problem is not a lack of awareness among frontline staff — it is a lack of systems, protocols, and accountability that would make disinfection a routine part of the workflow rather than an afterthought.
Part of the structural problem is time pressure. Modern radiology departments are under intense throughput pressure, scheduling patients back-to-back throughout the day. The Gutzeit study found that a complete disinfection of an MRI scanner and its receiver coils takes an average of 120 seconds — two minutes. Yet in practice, this two-minute window is rarely built into scheduling, and so it simply does not happen.
The misconception that placing a clean sheet on the scanner table between patients constitutes adequate infection control is widespread and dangerous. The CDC has explicitly stated that a clean sheet offers no protection against bacterial contamination — it merely covers the source rather than eliminating it.
6. What Good Practice Looks Like
The research literature, taken together, points toward a coherent set of best practices that would substantially reduce infection risk in diagnostic imaging facilities. None of them are technologically complex or prohibitively expensive; all of them require commitment and organisation.
Regular, systematic disinfection
Disinfection wipes should be used on all patient contact surfaces — table, headphones, coils, bore entrance, arm supports, and any other surface that patients touch — between every patient. The Gutzeit study demonstrated that a simple alcohol-free disinfection protocol can reduce mean bacterial colony counts from seven CFU per plate to essentially zero in two minutes. This is achievable in any department; it simply requires scheduling.
At the end of each scanning session, a more thorough disinfection including the scanner bore, control panels, keyboards, and chairs should be performed. Surfaces recommended for regular cleaning include: the CT bore, table, and wrap; the MRI table, coil surfaces, bore entrance, and any pressure-pad alarm devices; and all keyboard and touchscreen surfaces.
Staff attire and behaviour
Based on the balance of evidence, clinicians and radiographers performing direct patient contact in imaging departments should consider abandoning neckties and lanyards in clinical areas, in line with UK Department of Health guidance. Where ID must be worn, retractable badge clips attached to a breast pocket rather than a fabric lanyard represent a lower-risk alternative.
Mobile phones should be treated as potential fomites: kept out of immediate scanner rooms where possible, and cleaned regularly with disinfectant wipes if they must be carried. Hand hygiene — the bedrock of infection control — should be practised scrupulously before and after every patient contact, before donning and after removing gloves, and after any contact with equipment surfaces.
Scheduling and patient flow
Immunocompromised patients — those receiving chemotherapy, living with HIV/AIDS, or on post-transplant immunosuppression — should be scheduled at the beginning of the day or immediately after a thorough disinfection protocol, when surfaces are at their cleanest. This mirrors the approach used in surgical theatres, where high-risk patients are placed first on the operating list for exactly this reason.
Patients with known active infections should be scheduled at the end of the day’s list, with thorough disinfection performed immediately afterward, to minimise the risk of cross-contamination to subsequent patients.
Rethinking the animal question
The evidence from the Gutzeit study, and from basic hygiene principles, suggests that veterinary use of human MRI scanners — when accompanied by a mandatory post-use disinfection protocol — may actually improve overall hygiene compared to human-only use without systematic cleaning. Departments considering or already accommodating animal imaging should view the required disinfection protocol not as a cost of the arrangement, but as a benefit to human patients who follow.
7. Looking Forward
The landscape of infection control in radiology is beginning to change, driven by growing awareness, increasing regulatory attention to healthcare-associated infections, and — paradoxically — the COVID-19 pandemic, which forced many facilities to develop and implement surface disinfection protocols they had never previously considered.
Technologies with potential applications in diagnostic imaging infection control include UV-C light disinfection systems, which can be used to decontaminate scanner rooms between patients; antimicrobial surface coatings that can be applied to scanner components; and continuous environmental monitoring systems that provide real-time data on microbial load. None of these are yet in widespread use in radiology, but they represent the direction of travel.
The most important change, however, is cultural rather than technological. Radiology departments must come to see infection control not as a peripheral concern managed by someone else, but as a core patient safety responsibility — as central to their mission as image quality and reporting accuracy. The patients arriving in the scanner room include some of the most vulnerable in the entire hospital. They deserve the same standard of protection they would receive in any other clinical setting.
“The central question should perhaps not be whether we should allow dogs to undergo imaging in our hospitals, but rather we should focus on knowledge and perception of hygiene and understand what poses real danger and risk to our patients.” — Gutzeit et al., European Radiology, 2018
The invisible world of bacteria and viruses does not respect specialty boundaries or make allowances for scheduling pressure. It colonises neckties and lanyards, survives for weeks on foam padding, lurks in the folds of a scanner bore, and travels from patient to patient on the hands of staff who forgot to wash them. Addressing that world — systematically, rigorously, and without complacency — is not optional. For the neutropenic cancer patient heading into the scanner for their weekly monitoring, it may be a matter of life and death.
Key References
- Gutzeit, Andreas, et al. “Would it be safe to have a dog in the MRI scanner before your own examination? A multicenter study to establish hygiene facts related to dogs and men.” European radiology 29.2 (2019): 527-534.
- Jimenez, Yobelli A., and Sarah J. Lewis. “Infection prevention and control in the medical imaging environment: a scoping review.” Insights into Imaging 14.1 (2023): 121.
- Palmqvist, Charlotte, et al. “Surface contamination of CT and MRI equipment—a potential source for transmission of hospital-acquired infections.” Journal of Radiology Nursing 38.4 (2019): 254-260.
- Rothschild P. Preventing infection in MRI: Best practices for infection control in and around MRI suites. AuntMinnie / Radiology Today. 2008.
- ISID (International Society for Infectious Diseases). Infection Prevention and Control in the Radiology Department. Guide to Infection Control in the Healthcare Setting. 2021.
- Pace-Asciak, Pia, et al. “Health care professionals’ neckties as a source of transmission of bacteria to patients: a systematic review.” Canadian Medical Association Open Access Journal 6.1 (2018): E26-E30.
- Lopez, Pedro-Jose, et al. “Bacterial counts from hospital doctors’ ties are higher than those from shirts.” American journal of infection control 37.1 (2009): 79-80.
- Weber, R. L., et al. “Prospective study on the effect of shirt sleeves and ties on the transmission of bacteria to patients.” Journal of Hospital Infection 80.3 (2012): 252-254.
- Sartoretti, Thomas, et al. “Bacterial contamination of ultrasound probes in different radiological institutions before and after specific hygiene training: do we have a general hygienical problem?.” European radiology 27.10 (2017): 4181-4187.
- Delgado, Amanda, and Achuta Kumar Guddati. “Infections in hospitalized cancer patients.” World journal of oncology 12.6 (2021): 195.
- Centers for Disease Control and Prevention. Information for Patients Who Are Getting Chemotherapy: Preventing Infections in Cancer Patients. cdc.gov/cancer-preventing-infections. 2025.
- Klevans, R. M., et al. “Estimating Health Care—Associated Infections and Deaths in US Hospitals.” Public health reports 122.2 (2007): 160-66.
- Shteyer, Eyal, et al. “Modeling suggests that microliter volumes of contaminated blood caused an outbreak of hepatitis C during computerized tomography.” Plos one 14.1 (2019): e0210173.


{kind=link}